
Bone grafting has become an essential tool in modern dentistry and periodontal surgery, especially in restorative cases where the regeneration of alveolar bone is critical. Crushed bone allografts, including bone powder and bone granules, play a significant role in achieving predictable outcomes in Guided Bone Regeneration (GBR) and Guided Tissue Regeneration (GTR). The predictability, safety, and efficacy of these materials have made them a logical choice for many dentists.

In recent years, the use of bone grafts in dentistry and maxillofacial surgery has attracted the attention of many researchers and specialists. This article summarizes reviews and research articles that discuss the diverse applications and benefits of bone grafts in these fields. The goal of this article is to provide comprehensive and accurate information based on reliable scientific sources. A list of references is provided at the end of the article for further reading.
One of the most common challenges faced by dental surgeons is bone resorption in the jaw of patients requiring dental implants. Bone loss following tooth loss can lead to a significant reduction in the volume of surrounding bone due to the absence of the periodontium, which normally stimulates the alveolar bone to maintain its structure through the creation of additional blood vessels. Reduced bone dimensions can prevent satisfactory functional and aesthetic outcomes after dental implant placement. Despite efforts to produce implants with reduced height and width, the need to restore lost bone volume remains. Bone deficiency can only be repaired through bone grafting, which has now become an integral part of oral surgery, especially given the increasing awareness and expectations of patients regarding this type of treatment. Estimates suggest that half of all dental implant procedures involve the use of bone grafts.
Bone grafting is a common procedure in dentistry and dental implantology, used in various situations. Some common clinical procedures requiring bone grafting include dental implant placement, ridge augmentation, sinus lifts, socket preservation, and periodontal surgeries.
Under healthy conditions, small bone defects typically regenerate naturally; however, extensive bone defects, pathological fractures, and bone infections caused by periodontal issues or systemic diseases may impair the bone healing process, necessitating surgical intervention and the use of bone substitute materials.
Bone Grafting with Bone Powder and Other Bone Graft Products
Bone grafts, using bone powder and other bone graft products, are defined as tissues capable of filling bone voids and repairing or regenerating bone. These materials are either used alone or in combination with other substances to address bone defects. To date, many different bone regeneration materials, both synthetic and natural, have been used in orthopedic and maxillofacial surgery. An ideal bone graft should be biocompatible, absorbable, sterile, and easy to use, promoting bone regeneration through three key properties: osteogenesis, osteoconduction, and osteoinduction. The final characteristic of an ideal bone graft, osteoconduction, refers to the material’s ability to create a scaffold for the growth of blood vessels, osteoblasts, and host stem cells. Osteoinduction is the process by which bone formation is induced (i.e., new bone forms from bone cells in connective tissue or cartilage). Osteoconduction is defined as the process of bone growth from local bone tissue onto surfaces. Osteogenic materials are those that contain living cells capable of differentiating into bone.
Bone Substitutes in Dentistry
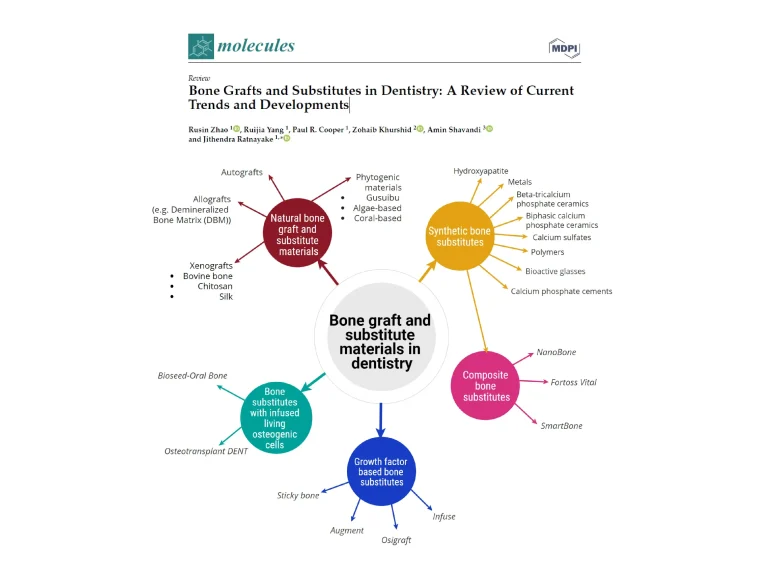
Various materials are available for bone grafting, and the choice of the ideal material depends on several factors, including material availability, defect size, graft size, shape, and volume, biomechanics, displacement, cost, ethical considerations, biological properties, and patient conditions. In this article, we examine different classifications of bone powders used in dentistry based on their origin or production methods.

Autograft Bone Powders
Autografts are considered the gold standard for bone grafting in medicine and dentistry. These materials meet many of the requirements for bone grafting as they are biocompatible, non-toxic, osteogenic, osteoinductive, and osteoconductive. These advantages are essential for rapid and efficient bone regeneration, particularly in critical-sized defects (>5 mm), where vascularization in the center of the defect is reduced. Healing time also depends on the material used, with autologous bone being the fastest and most osteogenic among all available materials.
Disadvantages of Autografts
Surgery at the bone harvesting site and potential complications, such as the risk of infection, are drawbacks of autografts. Additionally, the quantity and quality of donor bone may be insufficient due to age-related issues or medical conditions affecting the patient. In dentistry, due to the limited availability of intraoral bone and the need for additional surgery, this method is only used in critical cases such as jaw reconstruction, congenital bone defects, tumors, and bone defects larger than 5 mm. The need for additional surgery to harvest autogenous bone increases the inherent risks of any surgical procedure: pain, infection, scarring, and additional costs associated with hospitalization and a multidisciplinary team. Although autologous bone is still considered the best option, it has been increasingly replaced by other materials to reduce patient complications, treatment costs, surgical time, and postoperative recovery.
Xenograft Bone Powders in Dentistry
Xenografts, derived from animal sources, are widely used in dentistry and are well-documented materials that have been studied for over three decades. Their osteogenic properties stem from their inorganic structure, primarily composed of hydroxyapatite (HA), obtained by removing all organic components. Xenografts can come from various sources, with bovine and porcine sources being the most common. Other sources include horses, coral exoskeletons, and eggshells. One advantage of xenogenic materials is their chemical similarity to human bone, with a calcium/phosphorus ratio of 1.67, identical to that of human bone. Disadvantages include ethical, religious, and health concerns, such as the risk of disease transmission. Xenografts are among the most commonly used materials by dentists. Their effectiveness has been well-documented in several comparative studies with other materials, particularly autologous bone.
Some xenograft products are derived from bovine HA; one of their key features is their chemical similarity to human HA. Their calcium/phosphorus ratio of 1.67 matches that of human bone. Materials from other sources, such as horse bone, pig bone, coral exoskeletons, and even eggshells, have also been studied and commercialized. Each material has its unique properties, but in general, the advantages of these materials include low cost, high availability, and osteogenic properties. They are entirely composed of inorganic bone and lack any organic or cellular content. Some xenograft materials are also considered osteoinductive, although this is debated by some authors who argue that osteogenesis occurs only when cellular components, such as morphogenetic proteins, growth factors, or living cells, are present in the graft. Due to this osteoinductive property, animal-derived materials have been the subject of debate and controversy regarding their use in humans. As natural materials, they may retain some of their original properties after processing, such as certain cellular activities that confer osteoinductive properties. Although companies marketing xenogenic bone materials guarantee that their products are entirely free of organic matter, some plastic surgeons have detected proteins like collagen in certain xenografts after orthognathic surgery.
In another study, a foreign body reaction involving multinucleated cells surrounding particles of inorganic bovine bone was reported after histological analysis. These findings fuel the debate about the potential transmission of diseases that may occur when using these materials. Although such cases are rare, it is important to inform patients of this risk and alternative options. If xenogenic materials contain no organic components, their osteogenic capabilities are questionable. While many studies confirm their bone integration properties, other materials have been investigated to address the ethical and religious concerns associated with xenogenic materials and to improve manipulability, making the process easier for physicians and dentists. In addition to the mentioned issues, these materials require experienced handling. Since they are particulate, they require the use of a membrane to hold the particles in place and prevent connective tissue from infiltrating the area to be regenerated, complicating the procedure.
.
Synthetic Bone Powders and Materials
Synthetic bone graft products, or synthetic bone powders, offer several advantages over surgical methods for harvesting autogenous materials. These advantages include biocompatibility, osteoconductivity, injectability, moldability, ease of use, minimally invasive techniques, reduced scarring (since only the damaged area is surgically treated, and only one surgical procedure is required), and a lower risk of infection and other complications.
Another significant advantage of synthetic bone powders is their easy availability and mass producibility, unlike autogenous, allogeneic, or xenogenic materials. The increasing demand for bone regeneration materials has spurred extensive research into biomaterials to compensate for the limited availability of autogenous and allogeneic bone.
To date, several types of bioceramic materials have been developed as substitutes. Laboratory and clinical research has shown that these materials have effective osteoconductive properties. They have been successful in cases such as small to medium bone defects, ridge augmentation for implant placement, defects caused by periodontal disease, and maxillary sinus lifts.
Among ceramics, calcium phosphate-based materials are widely used due to their compositional similarity to natural bone and excellent biocompatibility. In addition to their granular form, these materials are also available as pastes, reducing application time and providing better moldability to the defect. However, the use of calcium phosphates for larger defects is limited due to their lack of osteogenic properties.
Therefore, much research has been conducted to improve the performance of these materials. It should be noted that synthetic materials alone cannot induce the formation of new bone, posing challenges for their use in critical-sized defects. To address this issue, additional components such as growth factors, cells, autogenous bone, and therapeutic elements are added to these materials to enhance their osteogenic properties.
This research field, known as tissue engineering, is based on three main elements:
- Scaffold or carrier material
- Biological components such as growth factors and drugs
- Cells
To select the most suitable material for a specific procedure, it is necessary to have a thorough understanding of the biological function of each material (e.g., osteogenesis, osteoinduction, and osteoconduction) and to consider the patient’s condition, as this is a fundamental criterion for the use of any type of bone graft. Bone grafts are evolving rapidly, and there has been much discussion about using synthetic bone grafts and bone substitutes instead of autologous, allogeneic, or even xenogeneic grafts.
Bioactive cements have been proposed as suitable alternatives to bone due to their moldability, self-hardening, and osteoconductivity. However, despite the widespread use of these biomaterials, the need to improve their mechanical properties remains. In the case of synthetic bone grafts, scaffolds not only provide mechanical support but also serve as a substrate for osteoblastic or osteoprogenitor cells to adhere, proliferate, and differentiate, forming new bone. These materials can also be used as carriers for other substances, including growth factors or drugs, or combined with other types of bone grafts to enhance or improve the bone formation process.
The most commonly used biomaterials among synthetic bone grafts include calcium phosphate-based cements, calcium phosphate ceramics, calcium sulfate, bioactive glasses, and polymers.
Calcium Phosphate Cements
Calcium phosphate-based materials have been used in dentistry and orthopedics since the 1980s and are now commercially available in various formulations. Calcium phosphate cements (CPCs) offer several advantages, including bioactivity, mass producibility, ease of use, and injectability to adapt to irregular bone defects. These materials also eliminate the inherent risks of autogenous and allogeneic grafts, such as donor site complications and infection risk.
The two main groups of CPCs are brushite and apatite. Apatite is formed from tetracalcium phosphate (TTCP) or β-TCP, while brushite is a byproduct of β-TCP or monocalcium phosphate monohydrate (MCPM).
Calcium Phosphate Ceramics
Calcium phosphate (CP) ceramic materials are available in granular or block forms with varying porosity and include HA, tricalcium phosphate (α-TCP and β-TCP), biphasic calcium phosphate (BCP), and amorphous calcium phosphate (ACP).
Hydroxyapatite (HA)
Hydroxyapatite (Ca10(PO4)6(OH)2) has significant osteoconductive properties due to its compositional similarity to the mineral component of natural bone and does not cause local or systemic toxicity, inflammation, or adverse immune reactions.
Tricalcium Phosphate
Beta-tricalcium phosphate (β-TCP) is highly regarded in biomaterials due to its dynamic stability in biological environments and greater absorbability at room temperature.
Calcium Sulfate
Calcium sulfate hemihydrate (CaSO4·1/2H2O), also known as plaster of Paris, has been used as a bone filler since the mid-1920s.
Bioactive Glasses (BGs)
Bioactive glasses are made from silica, calcium, and sodium oxide and interact with surrounding cells to aid bone regeneration.
Polymers
Research on polymers focuses on materials that can temporarily maintain the space needed for new bone formation and then degrade in the body.
Allograft Bone Powders in Dentistry
Allografts are grafts sourced from individuals of the same species. After thorough donor screening, these grafts are carefully processed and distributed by tissue banks. Allogeneic bone can exhibit both osteoinductive and osteoconductive properties and can be obtained from living or deceased donors of the same species but with different genotypes (in this case, human tissue). Fresh or frozen allogeneic bone typically shows better osteoinductive and mechanical properties but is associated with shorter storage times and risks of disease transmission or host immune reactions. Therefore, these products are usually processed by freeze-drying (lyophilization) and gamma irradiation for dental use. These grafts are available in various forms and sizes, including cortical, cancellous, or cortico-cancellous grafts. Allogeneic materials are considered a source of type I collagen and morphogenetic proteins, giving them osteoinductive capabilities. However, although they are derived from humans, they have different genetic compositions, raising concerns about immune rejection, blood compatibility, and the transmission of diseases or tumor cells. Products considered osteoinductive and osteoconductive do not have osteogenic properties, and their processing reduces their biological and mechanical characteristics. Due to the above issues, there is a need to develop processing and storage techniques that reduce risk and extend shelf life. Therefore, the properties of allogeneic bone grafts vary depending on the sterilization methods applied and the type of tissue. Available allogeneic materials can include fresh, frozen, or dried forms and can consist of cortical, cancellous, or cortico-cancellous bone tissue. In future articles, this topic will be discussed in detail. Physicians can use these products in various forms, from bone powder to larger bone pieces.
Classification of Allogeneic Bone Materials and Powders
Mineralized Bone Allograft
The most basic form of allogeneic bone graft is fresh, unprocessed bone. It can then be frozen (FFB), freeze-dried (FDBA, also known as MFDBA), or immediately grafted. Since processing techniques reduce the mechanical strength of allografts, fresh, unprocessed allografts have superior properties compared to processed bone. Unfortunately, due to fears of potential disease transmission and host immune reactions, fresh allografts are currently not very popular. The properties of mineralized allografts vary depending on whether they include cortical or cancellous bone tissue or both. In general, both cortical and cancellous allografts appear to have osteoconductive properties, with cortical bone being known for greater structural strength and better mechanical properties, leading to more favorable osteoconductive effects. Cortical bone is also denser and has slower resorption rates. For this reason, cortical allografts are typically used as whole bone sections, blocks, or pieces, while available forms of cancellous allografts include chips, wedges, and powders. Neither type of bone has osteogenic properties. Allogeneic bone blocks are usually composed of cancellous and cortical bone to benefit from both types of bone. Another notable aspect is the possible immune response to grafted tissues, leading to their rejection. To prevent this, a properly processed mineralized allogeneic bone should contain as few remaining donor cells or cellular debris as possible. This can be achieved by washing with water, ethanol, or mild solvents.
Demineralized Bone Matrix (DBM)
Since demineralized bone grafts, more commonly known as demineralized bone matrix (DBM), lack a mineralized matrix, the bone-inducing biochemical factors in the extracellular bone matrix, including BMPs, NCPs, and growth factors, become more biologically available. Therefore, DBM has superior osteoinductive properties compared to mineralized allogeneic bone, both cortical and cancellous. DBM, like other bone grafts, has no osteogenic ability. As mentioned, its osteogenic potential is significantly higher than that of conventional bone grafts due to increased access to osteogenic proteins in the extracellular bone matrix. After grafting, DBM slowly releases BMPs, further enhancing its osteogenic potential. While all available DBM materials appear to have osteogenic properties, there may be differences between them. This material also exhibits osteoconductive properties, although these are weaker than those of conventional mineralized bone grafts. Unfortunately, DBM itself is structurally weak, resulting in poor mechanical properties. Therefore, it is often combined with other grafts or even other grafting materials. DBM is commercially available in putty, blocks, particles, and powder forms.

Mineral and demineralized dental allograft bone powder
Decellularized Extracellular Matrix (dECM)
The term decellularized extracellular matrix refers to various types of allogeneic biomaterials made from human or animal tissue and obtained after removing cellular components that would normally cause immunogenicity. It has been shown that entire organs, such as lungs or hearts, can be decellularized for future replacement, not just bone tissue. The biological properties and physicochemical signals of dECM can be preserved despite the preparation process, making dECM a suitable three-dimensional scaffold for subsequent stem cell seeding. dECM can be obtained as a hydrogel, particles, or cellular matrix (after recellularization). Additionally, it has been used as a bioink in 3D bioprinting. dECM can generally be obtained in two ways: it can be extracted from tissue or from cells. dECM derived from bone tissue is obtained from an animal or human, living or deceased, and then undergoes a decellularization process. dECM derived from cells is created after culturing mesenchymal stem cells under in vitro conditions. To achieve the desired form of the resulting dECM, the culture is usually performed on a scaffold, such as hydroxyapatite.
Regen Allograft
The products of the Iranian Tissue Product Company (Regen Allograft) include a wide range of allogeneic bone grafts, the result of years of research and innovation. From dental bone powders to demineralized bone matrix (DBM) putty with bone regeneration capabilities, each of these products is designed with a focus on the needs of surgeons and patients. High processing quality, excellent biocompatibility, and appropriate performance in the surgical environment make these products an ideal choice for dental surgeons and maxillofacial specialists.
Our mission is to provide products that, while maintaining global quality and standards, offer innovative and effective treatments for patients. For this reason, our team is always striving to rely on advanced research and modern technologies to meet your needs and provide the best services.
References:
- Bone Grafts and Substitutes in Dentistry: A Review of Current Trends and Developments, 2023
- Allogenic Bone Graft in Dentistry: A Review of Current Trends and Developments, 2021
- Bone Grafts in Dental Medicine: An Overview of Autografts, Allografts and Synthetic Materials, 2023







